Official LAUSD Field Trip Permission Slip
Download or print the official form below
Fillable Digital Version
Use the form below for a digital version you can fill out and print
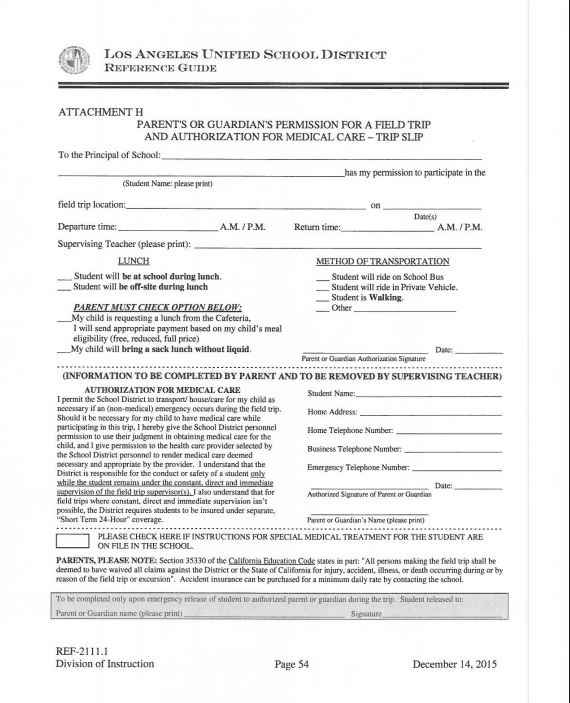
To the Principal of James Monroe High School:
(Student Name: please print)
Date(s)
LUNCH
PARENT MUST CHECK OPTION BELOW:
METHOD OF TRANSPORTATION
Parent or Guardian Authorization Signature
(INFORMATION TO BE COMPLETED BY PARENT AND TO BE REMOVED BY SUPERVISING TEACHER)
AUTHORIZATION FOR MEDICAL CARE
I permit the School District to transport/house/care for my child as necessary if an (non-medical) emergency occurs during the field trip. Should it be necessary for my child to have medical care while participating in this trip, I hereby give the School District personnel permission to use their judgment in obtaining medical care for the child, and I give permission to the health care provider selected by the School District personnel to render medical care deemed necessary and appropriate by the provider. I understand that the District is responsible for the conduct or safety of a student only while the student remains under the constant, direct and immediate supervision of the field trip supervisor(s). I also understand that for field trips where constant, direct and immediate supervision isn't possible, the District requires students to be insured under separate, "Short Term 24-Hour" coverage.
Authorized Signature of Parent or Guardian
PARENTS, PLEASE NOTE: Section 35330 of the California Education Code states in part: "All persons making the field trip shall be deemed to have waived all claims against the District or the State of California for injury, accident, illness, or death occurring during or by reason of the field trip or excursion". Accident insurance can be purchased for a minimum daily rate by contacting the school.
To be completed only upon emergency release of student to authorized parent or guardian during the trip. Student released to:
Signature
REF-2111.1
Division of Instruction
Page 54
December 14, 2015